

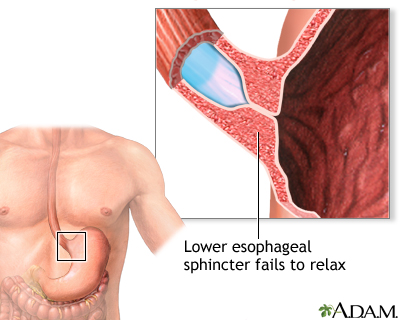
Achalasia is a rare disease of the muscle of the esophagus (swallowing tube). The term achalasia means "failure to relax" and refers to the inability of the lower esophageal sphincter (a ring of muscle between the lower esophagus and the stomach) to open and let food pass into the stomach. As a result, patients with achalasia have difficulty swallowing food.
How does the normal esophagus function?
The esophagus has three functional parts. The uppermost part is the upper esophageal sphincter, a specialized ring of muscle that forms the upper end of the tubular esophagus and separates the esophagus from the throat. The upper sphincter remains closed most of the time to prevent food in the main part of the esophagus from backing up into the throat. The main part of the esophagus is referred to as the body of the esophagus, a long, muscular tube approximately 20 cm (8 in) in length. The third functional part of the esophagus is the lower esophageal sphincter, a ring of specialized esophageal muscle at the junction of the esophagus with the stomach. Like the upper sphincter, the lower sphincter remains closed most of the time to prevent food and acid from backing up into the body of the esophagus from the stomach.
The upper sphincter relaxes with swallowing to allow food and saliva to pass from the throat into the upper esophageal body. The muscle in the upper esophagus just below the upper sphincter then contracts, squeezing food and saliva further down into the esophageal body. The ring-like contraction of the muscle progresses down the body of the esophagus, propelling the food and saliva towards the stomach. (The progression of the muscular contraction through the esophageal body is referred to as a peristaltic wave.). By the time the peristaltic wave reaches the lower sphincter, the sphincter is open, and the food passes into the stomach.
How is esophageal function abnormal in achalasia?
In achalasia there is an inability of the lower sphincter to relax and open to let food pass into the stomach. In at least half of the patients, the lower sphincter resting pressure (the pressure in the lower sphincter when the patient is not swallowing) also is abnormally high. In addition to the abnormalities of the lower sphincter, the muscle of the lower half of the esophagus does not contract normally, that is, peristaltic waves do not occur, and, therefore, food and saliva are not propelled down the esophagus and into the stomach. A few patients with achalasia have high-pressure waves in the lower esophageal body following swallows, but these high-pressure waves are not effective in pushing food into the stomach. These patients are referred to as having "vigorous" achalasia. These abnormalities of the lower sphincter and esophageal body are responsible for food sticking in the esophagus.
The cause of achalasia is unknown. Theories on causation invoke infection, heredity or an abnormality of the immune system that causes the body itself to damage the esophagus (autoimmune disease).
The esophagus contains both muscle and nerves. The nerves coordinate the relaxation and opening of the sphincters as well as the peristaltic waves in the body of the esophagus. Achalasia has effects on both the muscles and nerves of the esophagus; however, the effects on the nerves are believed to be the most important. Early in achalasia, inflammation can be seen under the microscope in the muscle of the lower esophagus, especially around the nerves. As the disease progresses, the nerves begin to degenerate and ultimately disappear, particularly the nerves that cause the lower esophageal sphincter to relax. Still later in the progression of the disease, muscle cells begin to degenerate, possibly because of the damage to the nerves. The result of these changes is a lower sphincter that cannot relax and muscle in the lower esophageal body that cannot support peristaltic waves. With time, the body of the esophagus stretches and becomes very enlarged (dilated).
What are the symptoms of achalasia?
The most common symptom of achalasia is difficulty swallowing (dysphagia). Patients typically describe food sticking in the chest after it is swallowed. Dysphagia occurs with both solid and liquid food. Moreover, the dysphagia is consistent, meaning that it occurs during virtually every meal.
Sometimes, patients will describe only a heavy sensation in their chest after eating that may force them to stop eating. Occasionally, pain may be severe and mimic heart pain. (Please read the Angina article on MedicineNet for more detail on different causes of chest pain).
Regurgitation of food that is trapped in the esophagus can occur, especially when the esophagus is dilated. If the regurgitation happens at night while the patient is sleeping, food can enter the throat and cause coughing and choking. If the food enters the trachea (windpipe) and lung, it can lead to pneumonia (aspiration pneumonia).
Because of the problem swallowing food, a large proportion of patients with achalasia lose weight.
What are the complications of achalasia?
The complications of achalasia include weight loss and aspiration pneumonia. There often is inflammation of the esophagus, called esophagitis, which is caused by the irritating effect of food and fluids that collect in the esophagus for prolonged periods of time. There may be esophageal ulcerations as well.
Of potential concern is the possibility that there is an increased occurrence of cancer of the esophagus in patients with achalasia. However, there is insufficient scientific evidence that achalasia increases a person's risk of developing esophageal cancer, so authorities are currently not recommending that patients with achalasia undergo regular upper gastrointestinal endoscopy for cancer surveillance.
The diagnosis of achalasia often is suspected on the basis of the history. Patients usually describe a progressive (worsening) of dysphagia for solid and liquid food over a period of many months to years. They may note regurgitation of food, chest pain, or loss of weight. Rarely, the first symptom is aspiration pneumonia.
Because patients typically will learn to compensate for their dysphagia by taking smaller bites, chewing well, and eating slowly, the diagnosis of achalasia often is delayed by months or even years. The delay in diagnosis of achalasia is unfortunate because it is believed that early treatment--before marked dilation of the esophagus occurs-can prevent esophageal dilation and its complications.
The dysphagia in achalasia also is different from the dysphagia of esophageal stricture (narrowing of the esophagus due to scarring) and esophageal cancer. In achalasia, dysphagia occurs with both solid and liquid food, whereas in esophageal stricture and cancer, the dysphagia typically occurs only with solid food.
X-ray studies
The diagnosis of achalasia usually is made by an x-ray study called a video-esophagram in which video x-rays of the esophagus are taken after barium is swallowed. The barium fills the esophagus, and the emptying of the barium into the stomach can be observed. In achalasia, the video-esophagram shows that the esophagus is dilated (enlarged or widened), with a characteristic tapered narrowing of the lower end, sometimes likened to a "bird's beak." In addition, the barium stays in the esophagus longer than normal before passing into the stomach.
Esophageal manometry
Another test, esophageal manometry, can demonstrate specifically the abnormalities of muscle function that are characteristic of achalasia, that is, the failure of the muscle of the esophageal body to contract with swallowing and the failure of the lower esophageal sphincter to relax. For manometry, a thin tube that measures the pressure generated by the contracting esophageal muscle is passed through the nose, down the back of the throat and into the esophagus. In a patient with achalasia, no peristaltic waves are seen in the lower half of the esophagus after swallows, and the pressure within the contracted lower esophageal sphincter does not fall with the swallow. An advantage of manometry is that it can diagnose achalasia early in its course at a time at which the video-esophagram may be normal.
Endoscopy
Endoscopy also is helpful in the diagnosis of achalasia although it can be normal early in achalasia. Endoscopy is a procedure in which a flexible fiberoptic tube with a light and camera on the end is swallowed. The camera provides direct visualization of the inside of the esophagus. One of the earliest endoscopic findings in achalasia is resistance as the endoscope is passed from the esophagus and into the stomach due to the high pressure in the lower esophageal sphincter. Later, endoscopy may reveal a dilated esophagus and a lack of peristaltic waves. Endoscopy also is important because it excludes the presence of esophageal cancer.
Two conditions can mimic achalasia, esophageal cancer and Chagas' disease of the esophagus. Both can give rise to video-esophageal and manometric abnormalities that are indistinguishable from achalasia. Fortunately, endoscopy usually can exclude the presence of cancer.
Chagas' disease is an infection caused by the parasite, Trypanosoma cruzi, and is limited to Central and South America. It is passed to humans through insect bites from the reduviid bug. The parasite is shed in the bug's feces at the time it is biting. Scratching the bite breaks the skin and allows the parasite to enter the body. The parasite spreads throughout the body but takes up primary residency in the muscles of the gastrointestinal tract, from the esophagus to the rectum, though it also often affects the muscle of the heart. In the gastrointestinal tract, the parasite causes degeneration of the nerves controlling the muscles and can lead to abnormal function anywhere in the gastrointestinal tract. When it affects the esophagus, the abnormalities are identical to those of achalasia.
Acute Chagas' disease occurs mostly in children. In those individuals who are seen at a much later time for problems swallowing, the acute illness is long-gone. The diagnosis of Chagas' disease can be suspected if there is involvement of other parts of the gastrointestinal tract, such as dilation of the small intestine or the colon and the heart. The best method for making a diagnosis is by serological tests looking for antibodies in the blood against the parasite.
Treatments for achalasia include oral medications, dilation or stretching of the lower esophageal sphincter (dilation), surgery to cut the sphincter (esophagomyotomy), and the injection of botulinum toxin (Botox) into the sphincter. All four treatments reduce the pressure within the lower esophageal sphincter to allow easier passage of food from the esophagus into the stomach.
Oral medications
Oral medications that help to relax the lower esophageal sphincter include groups of drugs called nitrates, e.g., isosorbide dinitrate (Isordil) and calcium-channel blockers, e.g., nifedipine (Procardia) and verapamil (Calan). Although some patients with achalasia, particularly early in the disease, have improvement of symptoms with medications, most do not. By themselves, oral medications are likely to provide only short-term and not long-term relief of the symptoms of achalasia, and many patients experience side-effects from the medications.
Dilation
The lower esophageal sphincter also may be treated directly by forceful dilation. Dilation of the lower esophageal sphincter is done by having the patient swallow a tube with a balloon on the end. The balloon is placed across the lower sphincter with the help of x-ray, and the balloon is blown up suddenly. The goal is to stretch--actually to tear--the sphincter. The success of forceful dilation has been reported to be between 60 and 95%. Patients in whom dilation is not successful can undergo further dilations, but the rate of success decreases with each additional dilation. If dilation is not successful, the sphincter may still be treated surgically. The main complication of forceful dilation is rupture of the esophagus, which occurs 5% of the time. Half of the ruptures heal without surgery, though patients with rupture who do not require surgery still must be followed closely and treated with antibiotics. The other half of ruptures require surgery. (Although surgery carries additional risk for the patient, surgery can repair the rupture as well as permanently treat the achalasia with esophagomyotomy.) Death following forceful dilation is rare. Dilation is fast, inexpensive compared with surgery, and requires only a short hospital stay.

Esophagomyotomy
The sphincter also can be cut surgically, a procedure called esophagomyotomy. The surgery can be done using a large abdominal incision or laparoscopically through small punctures in the abdomen. In general, the laparoscopic approach is used with uncomplicated achalasia. Alternatively, the surgery can be done with a large incision or laparoscopically through the chest. Esophagomyotomy is more successful than forceful dilation, probably because the pressure in the lower sphincter is reduced to a greater extent and more reliably; 80-90% of patients have good results. With prolonged follow-up, however, some patients develop recurrent dysphagia. Thus, esophagomyotomy does not guarantee a permanent cure. The most important side effect from the more reliable and greater reduction in pressure with esophagomyotomy, is reflux of acid (gastroesophageal reflux disease or GERD). In order to prevent this, the esophagomyotomy may be modified so that it doesn't completely cut the sphincter or the esophagomyotomy may be combined with anti-reflux surgery (fundoplication). Whichever surgical procedure is done, some physicians recommend life-long treatment with oral medications for acid reflux. Others recommend 24 hour esophageal acid testing with lifelong medication only if acid reflux is found.
Botulinum toxin
The newest treatment for achalasia is the endoscopic injection of botulinum toxin into the lower sphincter to weaken it. Injection is fast, nonsurgical, and requires no hospitalization. Treatment with botulinum toxin is safe, but the effects on the sphincter often last only for months, and additional injections with botulinum toxin may be necessary. Injection is a good option for patients who are very elderly or are at high risk for surgery, e.g., patients with severe heart or lung disease. It also allows patients who have lost substantial weight to eat and improve their nutritional status prior to "permanent" treatment with surgery. This may reduce post-surgical complications.
Achalasia At A Glance
- Achalasia is a rare disease of the muscle of the lower esophageal body and the lower esophageal sphincter.
- The cause of achalasia is unknown; however, there is degeneration of the esophageal muscle and, more importantly, the nerves that control the muscle.
- Common symptoms of achalasia include difficulty swallowing, chest pain, and regurgitation of food and liquid.
- Complications of achalasia include lung problems and loss of weight.
- Achalasia may increase the risk of cancer of the esophagus, but this is not clear.
- Achalasia can be diagnosed by x-ray, endoscopy, or esophageal manometry.
- Treatments for achalasia include oral medications, dilation or stretching of the esophagus, surgery, and injection of muscle-relaxing medicines (botulinum toxin) directly into the esophagus.
|
Bookmark this post:
|
|
0 comments
Post a Comment