
|
|










Liver Cancer At a Glance-Liver Cancer
- Liver cancer is the fifth most common cancer in the world and the majority of patients with liver cancer will die within one year as a result of the cancer.
- In the U.S., patients with associated cirrhosis caused by chronic hepatitis B or C infections, alcohol, and hemochromatosis are at the greatest risk of developing liver cancer.
- Patients with chronic liver disease (for example, hepatitis C virus, hepatitis B virus, or hemochromatosis) should avoid drinking alcohol, which can further increase their risk of developing cirrhosis and liver cancer.
- Many patients with liver cancer do not develop symptoms until the advanced stages of the tumor. When the patient does develop symptoms, the prognosis is usually poor.
- The combination of an imaging study (ultrasound, CT, or MRI scans) and an elevated blood level of alpha-fetoprotein most effectively diagnoses liver cancer.
- A liver biopsy can make a definitive diagnosis of liver cancer, but the procedure requires an expert liver pathologist and is not necessary for all patients.
- The natural history of liver cancer is quite variable, and depends on the stage of the tumor and the severity of the associated cirrhosis.
- Medical treatments for liver cancer, including chemotherapy, chemoembolization, ablation, and proton beam therapy, are not very effective.
- Surgical resection (removal) of the tumor may be very effective for a select group of individuals with liver cancer, specifically for those with small tumors and excellent liver function.
- For patients with small liver cancer and significant associated liver disease, liver transplantation offers the best chance for cure.
REFERENCES: Garden OJ, Rees M, Poston GJ, Mirza D, Saunders M, Ledermann J, Primrose JN, Parks RW. Guidelines for resection of colorectal cancer liver metastases. Gut. 2006 Aug;55 Suppl 3:iii1-8.
Brown DB, Geschwind JF, Soulen MC, Millward SF, Sacks D. Society of Interventional Radiology position statement on chemoembolization of hepatic malignancies. J Vasc Interv Radiol. 2006 Feb;17(2 Pt 1):217-23.
Bruix J, Sherman M; Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005 Nov;42(5):1208-36.
Medically Reviewed by Paul Oneill, MD, Board Certified Oncology
Prevention and Treatment of Liver Cancer?
![]() What's in the future?
What's in the future?
Prevention:Worldwide, the majority of liver cancer is associated with chronic hepatitis B virus infection. Today, however, all newborns are vaccinated against hepatitis B in China and other Asian countries. Therefore, the frequency of chronic hepatitis B virus in future generations will decrease.
Eventually, perhaps in three or four generations, hepatitis B virus will be totally eradicated, thereby eliminating the most common risk factor for liver cancer.
Some retrospective (looking back in time) studies suggest that patients with chronic hepatitis C who were treated with interferon were less likely to develop liver cancer than patients who were not treated. Interestingly, in these studies, interferon treatment seemed to provide this benefit, even to patients who had less than an optimal antiviral response to interferon. Still, it remains to be seen whether the risk of developing cirrhosis and liver cancer is significantly decreased in prospectively (looking ahead) followed patients who responded to interferon.
One Japanese study has reported that a retinoid derivative (a compound related to vitamin A) was effective in preventing recurrence of liver cancer after resection of the liver. As of now, this compound is not available in the U.S. It would be of great interest to study the use of this compound in conjunction with other palliative therapy for liver cancer.
Treatment
Unfortunately, there have been no significant new developments in the treatment of liver cancer. Medical therapy remains a disappointment. Scientists are working hard, however, to address this problem. For example, anti-angiogenesis compounds, which inhibit blood vessel formation, may hold promise in the treatment of liver cancer since this tumor depends on a rich blood supply. Also, different ways to deliver drugs or treatment to the tumors are being investigated. This includes attaching radioactive material to antibodies that are directed at specific targets in liver cancer cells (immunotherapy).
Proton beam therapy for Liver cancer-Treatment
 This technique is able to deliver high doses of radiation to a defined local area. Proton beam therapy is used in the treatment of other solid tumors as well. There are not much data yet regarding the efficacy of this treatment in liver cancer. The ideal patient is one with only asmall(<5 cm) solitary lesion. To have this procedure done, the patient actually is fitted with a body cast so that he or she can be placed in the identical position for each session.
This technique is able to deliver high doses of radiation to a defined local area. Proton beam therapy is used in the treatment of other solid tumors as well. There are not much data yet regarding the efficacy of this treatment in liver cancer. The ideal patient is one with only asmall(<5 cm) solitary lesion. To have this procedure done, the patient actually is fitted with a body cast so that he or she can be placed in the identical position for each session.
Therapy is conducted daily for 15 days. Preliminary data from the U.S. suggest similar effectiveness as seen with TACE or ablation therapy. It is not known, however, whether this type of radiation treatment prolongs the life of the patient. How do these various medical treatment procedures compare to each other? We really don't know because there are no head-to-head studies comparing chemotherapy, chemoembolization, ablation techniques, and proton beam therapy to each other.
Most reports deal with a heterogeneous group of patients who have undergone only one specific treatment procedure or another. Therefore, selection of a treatment option for a particular patient will depend primarily on the expertise of the doctors in the patient's area. Studies are also needed to evaluate combinations of these procedures (for example, proton beam and TACE)
Percutaneous ethanol (alcohol) injection method-Liver Cancer treatment
 Percutaneous ethanol (alcohol) injection for Liver Cancer treatment :In this technique for liver cancer, pure alcohol is injected into the tumor through a very thin needle with the help of ultrasound or CT visual guidance. Alcohol induces tumor destruction by drawing water out of tumor cells (dehydrating them) and thereby altering (denaturing) the structure of cellular proteins.
Percutaneous ethanol (alcohol) injection for Liver Cancer treatment :In this technique for liver cancer, pure alcohol is injected into the tumor through a very thin needle with the help of ultrasound or CT visual guidance. Alcohol induces tumor destruction by drawing water out of tumor cells (dehydrating them) and thereby altering (denaturing) the structure of cellular proteins.
It may take up to five or six sessions of injections to completely destroy the cancer. The ideal patient for alcohol injection has fewer than three liver cancer tumors, each of which is:
- well defined (distinct margins)
- less than 3 cm in diameter
- surrounded by a shell consisting of scar tissue (fibrous encapsulation)
- not near the surface of the liver
Liver cancer treatment::Additionally, patients with liver cancer undergoing alcohol injection should have no signs of chronic liver failure, such as ascites or jaundice. (Patients with liver failure would not be able to tolerate the alcohol injections.)
The most common side effect of alcohol injection in this liver cancer treatment method is leakage of alcohol onto the surface of the liver and into the abdominal cavity, thereby causing pain and fever. It is important that the location of the tumor relative to the adjacent blood vessels and bile ducts is clearly identified. The reason for needing to locate these structures is to avoid injuring them during the procedure and causing bleeding, bile duct inflammation, or bile leakage.
Liver Cancer Treatment-Radio frequency ablation therapy
 Liver Cancer Treatment using Radiofrequency ablation (RFA) therapyIn the U.S., RFA therapy has become the ablation (tissue destruction) therapy of choice among surgeons for liver cancer. The surgeon can perform this procedure laparoscopically (through small holes in the abdomen) or during open exploration of the abdomen.
Liver Cancer Treatment using Radiofrequency ablation (RFA) therapyIn the U.S., RFA therapy has become the ablation (tissue destruction) therapy of choice among surgeons for liver cancer. The surgeon can perform this procedure laparoscopically (through small holes in the abdomen) or during open exploration of the abdomen.
In some instances of this lever cancer treatment, the procedure can be done without opening the abdomen by just using ultrasound for visual guidance.
In RFA for treating liver cancer, heat is generated locally by a high frequency, alternating current that flows from the electrodes.In this lever cancer treatment a probe is inserted into the center of the tumor and the non-insulated electrodes, which are shaped like prongs, are projected into the tumor. The local heat that is generated melts the tissue (coagulative necrosis) that is adjacent to the probe. The probe is left in place for about 10 to 15 minutes. The whole procedure this liver cancer treatment is monitored visually by ultrasound scanning. The ideal size of an liver cancer tumor for RFA is less than 3 cm. Larger tumors may require more than one session. This treatment for liver cancer should be viewed as palliative (providing some relief), not curative.
Chemoembolization treatment of Liver Cancer-Liver cancer Treatment methods
 This technique takes advantage of the fact that liver cancer is a very vascular (contains many blood vessels) tumor and gets its blood supply exclusively from the branches of the hepatic artery. This procedure is similar to intra-arterial infusion of chemotherapy. But in TACE, there is the additional step of blocking (embolizing) the small blood vessels with different types of compounds, such as gelfoam or even small metal coils.
This technique takes advantage of the fact that liver cancer is a very vascular (contains many blood vessels) tumor and gets its blood supply exclusively from the branches of the hepatic artery. This procedure is similar to intra-arterial infusion of chemotherapy. But in TACE, there is the additional step of blocking (embolizing) the small blood vessels with different types of compounds, such as gelfoam or even small metal coils.
Thus, TACE has the advantages of exposing the tumor to high concentrations of chemotherapy and confining the agents locally since they are not carried away by the blood stream. At the same time, this technique deprives the tumor of its needed blood supply, which can result in the damage or death of the tumor cells.
The type and frequency of complications of TACE and intra-arterial chemotherapy are similar. The potential disadvantage of TACE is that blocking the feeding vessels to the tumor(s) may make future attempts at intra-arterial infusions impossible. Moreover, so far, there are no head-to-head studies directly comparing the effectiveness of intra-arterial infusion versus chemoembolization. In Japan, the chemotherapeutic agents are mixed with lipiodol. The idea is that since the tumor cells preferentially take up lipiodol, they would likewise take up the chemotherapy. This Japanese technique has not yet been validated in head-to-head comparisons with conventional TACE.
What are the benefits of TACE? In one large study involving several institutions in Italy, chemoembolization did not seem to be beneficial. Patients who did not undergo TACE lived as long as patients who received TACE, even though the tumors were more likely to shrink in size in patients who were treated. Does this mean that TACE or intra-arterial chemotherapy does not work? Maybe, maybe not.
Studies in Japan have shown that TACE can downstage liver cancer. In other words, the tumors shrank enough to lower (improve) the stage of the cancer. From the practical point of view, shrinking the tumor creates the option for surgery in some of these patients. Otherwise, these patients had tumors that were not operable (eligible for operation) because of the initial large size of their tumors. More importantly, these same studies showed an improvement in survival in patients whose tumors became considerably smaller. In the U.S., trials are underway to see whether doing TACE before liver transplantation increases patient survival as compared to liver transplantation without TACE.
It is safe to say that TACE or intra-arterial chemoinfusion are palliative treatment options for liver cancer. This means that these procedures can provide relief or make the disease less severe. However, they are not curative (do not result in a cure). Fewer than 50% of patients will have some shrinkage in tumor size. Further, they can be used only in patients with relatively preserved liver function. The reason for this is that these procedures, as mentioned previously, can lead to liver failure in individuals with poor liver function.
Liver cancer Chemotherapy Treatment-Liver cancer
 Systemic (entire body) chemotherapy
Systemic (entire body) chemotherapy
The most commonly used systemic chemotherapeutic agents are doxorubicin (Adriamycin) and 5-fluorouracil (5 FU). These drugs are used together or in combination with new experimental agents. These drugs are quite toxic and results have been disappointing. A few studies suggest some benefit with tamoxifen (Nolvadex) but just as many studies show no advantage.
Octreotide (Sandostatin) given as an injection was shown in one study to slow down the progression of large liver cancer tumors, but so far, no other studies have confirmed this benefit.
Hepatic arterial infusion of chemotherapy
The normal liver gets its blood supply from two sources; the portal vein (about 70%) and the hepatic artery (30%). However, liver cancer gets its blood exclusively from the hepatic artery. Making use of this fact, investigators have delivered chemotherapy agents selectively through the hepatic artery directly to the tumor. The theoretical advantage is that higher concentrations of the agents can be delivered to the tumors without subjecting the patients to the systemic toxicity of the agents.
In reality, however, much of the chemotherapeutic agents does end up in the rest of the body. Therefore, selective intra-arterial chemotherapy can cause the usual systemic (body-wide) side effects. In addition, this treatment can result in some regional side effects, such as inflammation of the gallbladder (cholecystitis), intestinal and stomach ulcers, and inflammation of the pancreas (pancreatitis). Liver cancer patients with advanced cirrhosis may develop liver failure after this treatment. Well then, what is the benefit of intra-arterial chemotherapy? The bottom line is that fewer than 50% of patients will experience a reduction in tumor size.
An interventional radiologist (one who does therapeutic procedures) usually carries out this procedure. The radiologist must work closely with an oncologist (cancer specialist), who determines the amount of chemotherapy that the patient receives at each session. Some patients may undergo repeat sessions at 6 to 12 week intervals. This procedure is done with the help of fluoroscopy (type of x-ray) imaging. A catheter (long, narrow tube) is inserted into the femoral artery in the groin and is threaded into the aorta (the main artery of the body). From the aorta, the catheter is advanced into the hepatic artery. Once the branches of the hepatic artery that feed the liver cancer are identified, the chemotherapy is infused. The whole procedure takes one to two hours, and then the catheter is removed.
The patient generally stays in the hospital overnight for observation. A sandbag is placed over the groin to compress the area where the catheter was inserted into the femoral artery. The nurses periodically check for signs of bleeding from the femoral artery puncture. They also check for the pulse in the foot on the side of the catheter insertion to be sure that the femoral artery is not blocked as a result of the procedure. (Blockage would be signaled by the absence of a pulse.)
Generally, the liver tests increase (get worse) during the two to three days after the procedure. This worsening of the liver tests is actually due to death of the tumor (and some non-tumor) cells. The patient may experience some post-procedure abdominal pain and low-grade fever. However, severe abdominal pain and vomiting suggest that a more serious complication has developed. Imaging studies of the liver are repeated in six to 12 weeks to assess the size of the tumor in response to the treatment.Treatments of Liver Cancer-Options for liver cancer treament
 The treatment options are dictated by the stage of liver cancer and the overall condition of the patient. The only proven cure for liver cancer is liver transplantation for a solitary, small tumor. Now, many physicians may dispute this statement. They may argue that a small tumor can be surgically removed (partial hepatic resection) without the need for a liver transplantation.
The treatment options are dictated by the stage of liver cancer and the overall condition of the patient. The only proven cure for liver cancer is liver transplantation for a solitary, small tumor. Now, many physicians may dispute this statement. They may argue that a small tumor can be surgically removed (partial hepatic resection) without the need for a liver transplantation.
Moreover, they may claim that the one and three year survival rates for resection are perhaps comparable to those for liver transplantation.
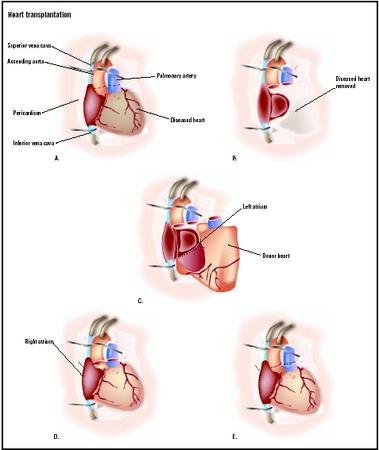
However, most patients with liver cancer also have cirrhosis of the liver and would not tolerate liver resection surgery. But, they probably could tolerate the transplantation operation, which involves removal of the patient's entire diseased liver just prior to transplanting a donor liver. Furthermore, many patients who undergo hepatic resections will develop a recurrence of liver cancer elsewhere in the liver within several years. In fact, some experts believe that once a liver develops liver cancer, there is a tendency for that liver to develop other tumors at the same time (synchronous multicentric occurrence) or at a later time (metachronous multicentric occurrence).
The results of the various medical treatments of liver cancer(chemotherapy, chemoembolization, ablation, and proton beam therapy) remain disappointing. Moreover, for reasons noted earlier (primarily the variability in natural history), there have been no systematic study comparisons of the different treatments. As a result, individual patients will find that the various treatment options available to them depend largely on the local expertise.
How do we know if a particular treatment of liver cancer worked for a particular patient of liver cancer? Well, hopefully, the patient will feel better. However, a clinical response to treatment of liver caner is usually defined more objectively. Thus, a response is defined as a decrease in the size of the tumor on imaging studies along with a reduction of the alpha-fetoprotein in the blood, if the level was elevated prior to treatment.
Symptoms of Liver Cancer-Indiaction's of liver cancer
 The initial symptoms (the clinical presentations) of liver cancer are variable. In countries where liver cancer is very common, the cancer generally is discovered at a very advanced stage of disease for several reasons. For one thing, areas where there is a high frequency of liver cancer are generally developing countries where access to healthcare is limited.
The initial symptoms (the clinical presentations) of liver cancer are variable. In countries where liver cancer is very common, the cancer generally is discovered at a very advanced stage of disease for several reasons. For one thing, areas where there is a high frequency of liver cancer are generally developing countries where access to healthcare is limited.
For another, screening examinations for patients at risk for developing liver cancer are not available in these areas. In addition, patients from these regions actually have more aggressive liver cancer disease. In other words, the tumor usually reaches an advanced stage and causes symptoms more rapidly. In contrast, patients in areas of low liver cancer frequency tend to have liver cancer tumors that progress more slowly and, therefore, remain without symptoms longer.
Abdominal pain is the most common symptom of liver cancer and usually signifies a very large tumor or widespread involvement of the liver. Additionally, unexplained weight loss or unexplained fevers are warning signs of liver cancer in patients with cirrhosis. These symptoms are less common in individuals with liver cancer in the U.S. because these patients are usually diagnosed at an earlier stage. However, whenever the overall health of a patient with cirrhosis deteriorates, every effort should be made to look for liver cancer.
A very common initial presentation of liver cancer in a patient with compensated cirrhosis (no complications of liver disease) is the sudden onset of a complication. For example, the sudden appearance of ascites (abdominal fluid and swelling), jaundice (yellow color of the skin), or muscle wasting without causative (precipitating) factors (for example, alcohol consumption) suggests the possibility of liver cancer. What's more, the cancer can invade and block the portal vein (a large vein that brings blood to the liver from the intestine and spleen). When this happens, the blood will travel paths of less resistance, such as through esophageal veins. This causes increased pressure in these veins, which results in dilated (widened) veins called esophageal varices. The patient then is at risk for hemorrhage from the rupture of the varices into the gastrointestinal tract. Rarely, the cancer itself can rupture and bleed into the abdominal cavity, resulting in bloody ascites.
On physical examination, an enlarged, sometimes tender, liver is the most common finding. Liver cancers are very vascular (containing many blood vessels) tumors. Thus, increased amounts of blood feed into the hepatic artery (artery to the liver) and cause turbulent blood flow in the artery. The turbulence results in a distinct sound in the liver (hepatic bruit) that can be heard with a stethoscope in about one quarter to one half of patients with liver cancer. Any sign of advanced liver disease (for example, ascites, jaundice, or muscle wasting) means a poor prognosis. Rarely, a patient with liver cancer can become suddenly jaundiced when the tumor erodes into the bile duct. The jaundice occurs in this situation because both sloughing of the tumor into the duct and bleeding that clots in the duct can block the duct.
In advanced liver cancer, the tumor can spread locally to neighboring tissues or, through the blood vessels, to elsewhere in the body (distant metastasis). Locally, liver cancer can invade the veins that drain the liver (hepatic veins). The tumor can then block these veins, which results in congestion of the liver. The congestion occurs because the blocked veins cannot drain the blood out of the liver. (Normally, the blood in the hepatic veins leaving the liver flows through the inferior vena cava, which is the largest vein that drains into the heart.) In African patients, the tumor frequently blocks the inferior vena cava. Blockage of either the hepatic veins or the inferior vena cava results in a very swollen liver and massive formation of ascites. In some patients, as previously mentioned, the tumor can invade the portal vein and lead to the rupture of esophageal varices.
Regarding the distant metastases, liver cancer frequently spreads to the lungs, presumably by way of the blood stream. Usually, patients do not have symptoms from the lung metastases, which are diagnosed by radiologic (x-ray) studies. Rarely, in very advanced cases, liver cancer can spread to the bone or brain.
|
|