

Introduction to anaphylaxis
Anaphylaxis refers to a rapidly developing and serious allergic reaction that affects a number of different areas of the body at one time. Severe anaphylactic reactions can be fatal. Most people experience allergy symptoms only as a minor annoyance. However, a small number of people are susceptible to a reaction that can lead to shock or even death.
Anaphylaxis is often triggered by substances that are injected or ingested and thereby gain access into the blood stream. An explosive reaction involving the skin, lungs, nose, throat, and gastrointestinal tract can then result. Although severe cases of anaphylaxis can occur within seconds or minutes of exposure and be fatal if untreated, many reactions are milder and can be ended with prompt medical therapy.
What does anaphylaxis mean?
To fully understand this term, we need to go back almost 100 years. The story begins on a cruise aboard Prince Albert I of Monaco's yacht. The Prince had invited two Parisian scientists to perform studies on the toxin produced by the tentacles of a local jellyfish, the Portuguese Man of War. Charles Richet and Paul Portier were able to isolate the toxin and tried to vaccinate dogs in the hope of obtaining protection, or "prophylaxis," against the toxin. They were horrified to find that subsequent very small doses of the toxin unexpectedly resulted in a new dramatic illness that involved the rapid onset of breathing difficulty and resulted in death within 30 minutes. Richet and Portier termed this "anaphylaxis" or "against protection." They rightly concluded that the immune system first becomes sensitized to the allergen over several weeks and upon re-exposure to the same allergen may result in a severe reaction. An allergen is a substance that is foreign to the body and can cause an allergic reaction in certain people.
Allergy Facts
- The first documented case of presumed anaphylaxis occurred in 2641 B.C. when Menes, an Egyptian pharaoh, died mysteriously following a wasp or hornet sting. Later, in Babylonian times, there are two distinct references to deaths due to wasp stings.
- Charles Richet was awarded the Nobel Prize in 1913 for his work on anaphylaxis.
Richet went on to suggest that the allergen must result in the production of a substance, which then sensitized the dogs to react in such a way upon re-exposure. This substance turned out to be IgE.
In the first part of the 20th century, anaphylactic reactions were most commonly caused by tetanus diphtheria vaccinations made from horse serum. Today, human serum is used for tetanus prevention, and the most common causes of anaphylaxis are now penicillin and other antibiotics, insect stings, and certain foods.
Allergy Fact
In 1956, Mary Hewitt Loveless showed that the injection of wasp venoms could cause anaphylaxis in individuals allergic to wasps. She subsequently used wasp extracts to successfully immunize such individuals.
How common is anaphylaxis?
The exact prevalence of anaphylaxis is unknown. The available statistics probably underestimate the true frequency because reactions are not always reported. Milder reactions may be attributed to an asthma attack or a sudden episode of hives. More serious, fatal episodes might be reported as a heart attack since the indicative signs of hives, swollen throat, and asthma can fade quickly. Thus, it is quite possible that even the true incidence of fatalities due to anaphylaxis is both under- recognized and under-reported. The importance of awareness, early recognition, and prompt treatment of this disorder must be stressed.
What are common causes of anaphylaxis?
The causes of anaphylaxis are divided into two major groups:
- IgE mediated: This form is the true anaphylaxis that requires an initial sensitizing exposure, the coating of mast cells and basophils (cells in the blood and tissue that secrete the substances that cause allergic reactions, known as mediators) by IgE, and the explosive release of chemical mediators upon re-exposure.
- Non-IgE mediated: These reactions, the so called "anaphylactoid" reactions, are similar to those of true anaphylaxis, but do not require an IgE immune reaction. They are usually caused by the direct stimulation of the mast cells and basophils. The same mediators as occur with true anaphylaxis are released and the same effects are produced. This reaction can happen, and often does, on initial as well as subsequent exposures, since no sensitization is required.
The terms anaphylaxis and anaphylactoid (meaning "like anaphylaxis") are both used to describe this severe, allergic reaction. Anaphylaxis is used to describe reactions that are initiated by IgE and anaphylactoid is used in reference to reactions that are not caused by IgE. The effects of the reactions are the same, however, and are generally treated in the same manner. Often, they can not be distinguished initially.
Although it may appear that IgE mediated anaphylaxis occurs upon a first exposure to a food, drug, or insect sting, there must have been a prior, and probably unwitting, sensitization from a previous exposure. You may not remember an uneventful sting or be aware of "hidden" allergens in foods.
What are the signs of anaphylaxis?
It is worth mentioning a few general observations regarding the features of anaphylactic reactions. Be aware, however, that these guidelines are not always consistent or reliable for a particular individual.
- The severity of the reaction varies from person to person.
- Subsequent reactions to the same trigger are typically similar in nature.
- The more rapid the onset of symptoms, the more severe the reaction is likely to be.
- A history of allergic disease (rhinitis, eczema, asthma) does not increase the risk of developing IgE mediated anaphylaxis, but it does incline the person to a non-IgE mediated reaction.
- Underlying asthma may result in a more severe reaction and can be more difficult to treat.
- The risk of anaphylaxis may diminish over time if there are no repeated exposures or reactions. However, a person at risk should always expect the worst and be prepared.
What are anaphylaxis symptoms?
The symptoms of an anaphylactic reaction may occur within seconds of exposure, or be delayed 15 to 30 minutes, or even an hour or more after exposure (typical of reactions to aspirin and similar drugs). Early symptoms are often related to the skin and include:
- Flushing (warmth and redness of the skin),
- itching (often in the groin or armpits), and
- hives.
These symptoms are often accompanied by:
- a feeling of "impending doom,"
- anxiety, and
- sometimes a rapid, irregular pulse.
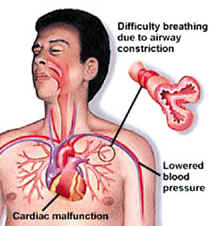
Frequently following the above symptoms, throat and tongue swelling results in hoarseness, difficulty swallowing, and difficulty breathing.
Symptoms of rhinitis (hay fever) or asthma may occur causing:
- a runny nose,
- sneezing, and wheezing, which may worsen the breathing difficulty,
- vomiting, diarrhea, and stomach cramps may develop.
About 25% of the time, the mediators flooding the blood stream cause a generalized opening of capillaries (tiny blood vessels) which results in a drop in blood pressure, lightheadedness, or even loss of consciousness. These are the typical features of anaphylactic shock.
What happens after the symptoms begin?
There are three possible outcomes:
- The signs and symptoms may be mild and fade spontaneously or be quickly ended by administering emergency medication. In this outcome, the symptoms do not subsequently recur from this particular exposure.
- After initial improvement, the symptoms may recur within 4 to 12 hours (late phase reaction) and require additional treatment and close observation. Recent evidence suggests that a late phase reaction occurs in fewer than 10% of cases.
- Lastly, the reaction may be persistent and more severe, thus requiring intensive medical treatment and hospitalization. This may occur up to 20% of the time with certain exposures.
Epinephrine, which is also known as "adrenaline," is a drug that acts immediately to cause the blood vessels to contract, thereby preventing fluid leakage. It is one of the medications frequently used to treat anaphylaxis. Epinephrine also helps relax the bronchial tubes, thus relieving breathing difficulty. It also lessens stomach cramps and stops itching and hives. More importantly, epinephrine helps prevent the release of more mediators of the allergic reaction. In addition to epinephrine, other medications and IV fluids and oxygen will probably be administered as well. The choice of interventions will depend on the severity of the reaction the patient experiences.
Are there any disorders that appear similar to anaphylaxis?
Several disorders may appear similar to anaphylaxis. Fainting (vaso-vagal reaction) is the reaction that is most likely to be confused with anaphylaxis. The key differences are that in a fainting episode, the affected person has a slow pulse, cool and pale skin, and no hives or difficulty breathing. Other conditions, such as heart attacks, blood clots to the lungs, septic shock, and panic attacks can also be confused with anaphylaxis.
How is anaphylaxis diagnosed?
Once you think that you might have had an anaphylactic reaction, the first order of business is to seek emergency care. Once the acute reaction has been treated you should follow-up with your doctor who will probably recommend seeing an allergist. The allergist will assess whether or not the reaction was indeed allergic in nature. Usually, a careful and detailed medical history and selected blood or skin tests can identify the cause. Be prepared to recall your activities before the event, the food and medications you ingested, and whether or not you had any contact with rubber products.
Table 1: The Common Causes of Anaphylaxis
| Causes - IgE Mediated | Examples |
|---|---|
| Medications | Penicillin, Cephalosporin, Anesthetics, Streptokinase, Others |
| Insect Stings | Hornet, Wasp, Yellow Jacket, Honey Bee, Fire Ant |
| Foods | Peanuts, Treenuts, Fish, Shellfish, Eggs, Milk, Soy, Wheat |
| Vaccines | Allergy Shots, Egg and Gelatin based vaccines |
| Hormones | Insulin, Possibly Progesterone |
| Latex | Rubber Products |
| Animal/Human Proteins | Horse Serum (used in some snake anti-venoms) |
| Causes - Non IgE Mediated | Examples |
|---|---|
| Medication | Non-steroidal Anti-inflammatories (Aspirin, Motrin, etc.), Morphine, Muscle Relaxants (Robaxin, Norflex, and others), Gamma Globulin |
| X-ray Dye | |
| Preservatives | Sulfites |
| Physical | Exercise, Heat-Induced Urticaria (Hives), Cold- Induced Urticaria |
| Idiopathic | Unknown Cause |
How do we manage anaphylaxis?
The optimal management of anaphylaxis saves lives. An affected or at-risk person must be aware of possible triggers and early warning signs. If you are prone to these reactions, you must be familiar with the use of emergency anaphylaxis treatment kits and always have them with you. Emergency measures and prevention are central to management. As always, allergic diseases are best treated by avoidance measures, which will be reviewed in detail below.
What are emergency measures for anaphylaxis?
If you suspect that you or someone you are with is having an anaphylactic reaction, the following are important first aid measures. In general, try to perform these in the order that they are presented.
- Call emergency services or 911 IMMEDIATELY.
- If the patient has an epi-pen, inject epinephrine immediately. The shot is given into the outer thigh and can be administered through light fabric. Rub the site to improve absorption of the drug.
- Place a conscious person lying down and elevate the feet if possible.
- Stay with the person until help arrives.
- If trained, begin CPR if the person stops breathing or doesn't have a pulse.
Allergy Assist
Shots of epinephrine can be given through light clothing such as trousers, skirts, or stockings. Heavy garments may have to be removed prior to injecting. Only inject epinephrine if the patient has a history of anaphylactic reactions or under guidance of a healthcare provider.
After 10 to 15 minutes, if the symptoms are still significant, you can inject another dose of epinephrine if available. Even after the reaction subsides you need to go to an emergency department immediately. Other treatments may be given, such as oxygen, intravenous fluids, breathing medications, and possibly more epinephrine. Steroids and antihistamines may be given but these are often not helpful initially and do not take the place of epinephrine. However, they may be more useful in preventing a recurrent delayed reaction.
Do not be surprised if epinephrine makes you feel shaky and causes a rapid, pounding pulse. These are normal side effects and are not dangerous except for those with severe heart problems.

Two situations deserve special attention at this point since they are not covered elsewhere but are particularly interesting.
- In the 1970's, it was noted that exercise could cause anaphylaxis. Exercise-induced anaphylaxis (EIA) usually occurs with prolonged, strenuous exercise. Conditioned athletes such as marathon runners are frequently affected. The reaction may occur while exercising shortly after eating a meal, after eating specific foods (for example, lettuce, shellfish, or celery) or after taking aspirin. It appears as though food or aspirin loads the gun and exercise pulls the trigger. Early symptoms are usually flushing and itching, which may progress to other typical symptoms of anaphylaxis if the exercise continues. Pre-medication with antihistamines or other drugs does not consistently prevent EIA. Exercise avoidance is the most effective treatment. If this is not feasible, exercising with a "buddy" and carrying emergency kits is mandatory.
- When no cause can be found for anaphylaxis, it is termed idiopathic. Recent reports suggest that 25% of all episodes of anaphylaxis are idiopathic. Many of those affected have underlying allergy or asthma conditions. Extensive allergy testing for foods may uncover an unusual food allergy that is responsible for these reactions. For frequent episodes of anaphylaxis, your physician may recommend a combination of antihistamine, cortisone, and a medication to widen the airways of the lungs (bronchial dilator) to help reduce the severity of attacks.
Can anaphylaxis be prevented?
Preventing anaphylaxis is the ideal form of treatment. However, that may not always be easy since insect stings are frequently unanticipated and allergic foods are often hidden in a variety of different preparations. A consultation with an allergist is vital in helping you identify the trigger(s) and providing you with information and instruction on how to best avoid them. You will learn how to use emergency kits and how to become prepared for any reaction in the future.
These are three situations in which preventive treatment might be offered by the allergist.
- Allergy shots may be suggested to some people with wasp, yellow jacket, hornet, honey bee, or fire ant reactions. This form of treatment gives 98% protection against the first four insect reactions, though somewhat less protection against fire ant reactions.
- Pre-medication is most helpful in preventing anaphylaxis from x-ray dyes. Alternative dyes that are less likely to cause reactions may be available.
- Desensitization to problematic medications is often effective. This process is accomplished by gradually increasing the amount of the medication given under controlled conditions. Sensitivities to penicillin, sulfa drugs, and insulin have been successfully treated in this way.
Anyone known to be at risk for anaphylaxis should wear a Medic-Alert bracelet that clearly states the allergic trigger, the risk of anaphylaxis, and the availability of an epinephrine kit.
Allergy Assist
People with anaphylaxis to medications should take new medications by mouth whenever possible since the risk of anaphylaxis is higher with injections.
Table 2: Basic Avoidance Measures for Anaphylaxis
| Trigger | Avoidance Principle |
|---|---|
| |
| |
| |
|
Since avoidance is not fail safe, a person at risk for an anaphylactic reaction must be adequately prepared in an emergency to handle a reaction. It is recommended that everyone at risk carry epinephrine injection kits designed for self-administration. These kits are available by prescription only and come in two forms:
- Epi-pen is a spring-loaded automatic syringe that delivers a predetermined dose (0.3mg) when the tip is pressed hard for several seconds. An Epi-pen junior is available for children under 33 pounds and contains half of the dose.
- Ana-kit contains a preloaded syringe and needles with two 0.3mg doses of epinephrine. These are injected under the skin or into the muscle of the thigh. An antihistamine, alcohol swab, and a tourniquet are included in the kit.
Here are some important points to remember regarding the kits:
- Ask you doctor to explain the use of the kit carefully and practice with the demonstrator kit.
- Check expiration dates and replace outdated kits.
- Keep kits out of direct sunlight, which may affect the drug.
- Additional kits should be brought to school or work.
- Always have kits with you or readily available.
- Make sure that your friends, relatives, exercise buddies, and co-workers are aware of your condition and know what to do in case of a reaction.
Anaphylaxis At A Glance
- Anaphylaxis is the most severe allergic reaction and is potentially life threatening.
- Anaphylaxis is rare. The vast majority of people will never have an anaphylactic reaction.
- The most common causes of anaphylaxis include drugs, such as penicillin, insect stings, foods, x-ray dye, latex, and exercise.
- The symptoms of anaphylaxis may vary from hives, tongue swelling, and vomiting, to shock.
- If you are at risk, avoidance is the best form of treatment.
- If you have a history of serious allergic reaction, always have an epinephrine kit available - it could save your life.
|
Bookmark this post:
|
|
0 comments
Post a Comment